The temporalis muscle is located in the temple area of the skull. It originates on the temporal lines on the parietal bone of the skull, and inserts on the coronoid process of the mandible. It’s main action is to close the jaw. The posterior and middle fibres bilaterally retrude the mandible. Acting individually, this muscle will deviate the mandible to the same side. Trigger points in this muscle refer into the teeth causing hypersensitivity, and into and above the eye and temple, causing headaches.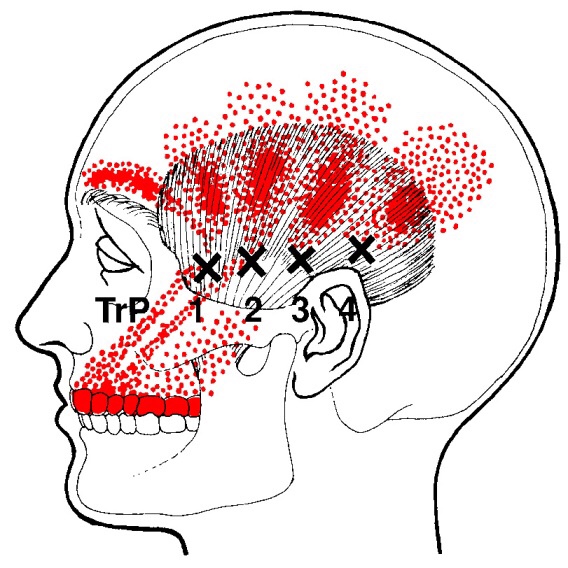
Interesting News
Trigger points in the lateral pterygoid
The lateral pterygoid muscle plays an important role in prober jaw function. It originates on the greater wing of the sphenoid bone and the lateral pterygoid plate, and inserts on the condyloid process of the mandible. It’s action is to pull the head of the mandibular condyle out of the mandibular fossa while opening the jaw. When trigger points develop they refer pain into the temporal mandibular joint and maxillary sinus. This referral is commonly mistaken for TM arthritis. In addition to the referral pain, trigger points in this muscle can also effect proper movement of the jaw.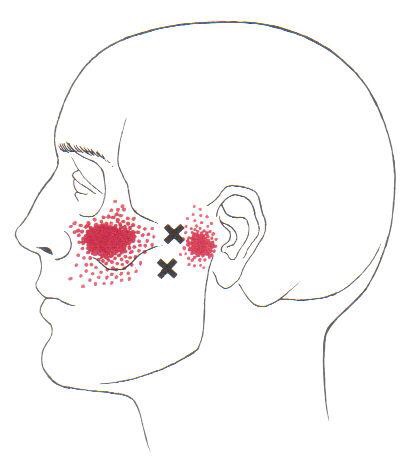

Spring Cleaning Tips
If you plan on doing a bit of spring cleaning soon, here is our friendly safety reminder: Don’t forget that some chores are a workout, so stretch accordingly before and after. Also, be mindful of your posture throughout your cleaning.
Keep a neutral spine, bend at your knees when lifting heavy items, and never twist your back at unhealthy angles.
Trigger points in the serratus anterior
The serratus anterior muscle is located along the sides of the ribs. It originates on the outer surface of the upper 8-9ribs, and inserts on the medial border of the scapula. This muscle acts on the scapula in several different ways. First it rotates the scapula to turn the glenoid fossa upward. It also protracted and elevates the scapula. And lastly it helps to prevent wining. This muscle is often shortened from prolonged sitting and work on a computer. Active trigger points in this muscle refer pain locally around the trigger point with spillover down the inside of the arm. Pain can also radiate into the inferior angle of the scapula. 
Trigger points in the iliopsoas muscle
This muscle originates on the bodies and disks of T12-L5 and the inner ilium. It inserts on the lesser trochanter of the femur. The psoas flexes the hip when the spine is fixed. When the leg is fixed it extends the lumbar spine increasing lumbar lordosis. This Muscle is often chronically shortened due to inactivity and sitting posture. When trigger points are present they will refer pain primarily to the lower lumbar area and the sacrum as well as into the anterior thigh. Trigger points in the iliopsoas muscle can mimic appendicitis.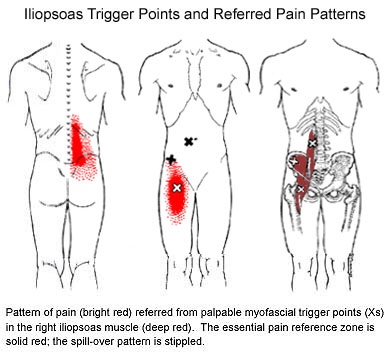
Trigger points in the piriformis muscle
The piriformis muscle is a small muscle deep to glute max and lies over top of the sciatic nerve. It originates on the anterior sacrum, and inserts on the greater trochanter of the femur. It’s main action is to laterally rotate the femur. When trigger points developed in this muscle they will refer pain into the sacro-iliac region, across the posterior hip and down the leg. This muscle can also be a cause of sciatic nerve irritation if it gets tight, causing “sciatica” symptoms. 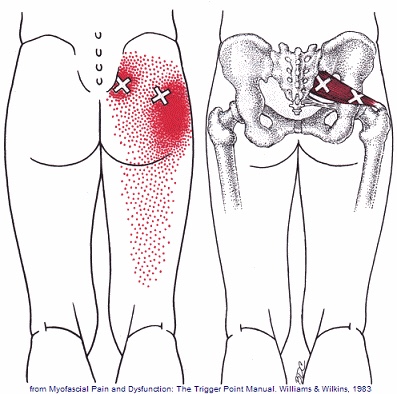
Osteoporosis and Compression Fractures
Most of the tissues in our body are in a constant state of rejuvenation, wherein old cells are removed to be replaced by new. In our skeleton, when the production of new bone cannot keep up with the rate of tear down, our bones become progressively thinner and weaker in a process called “osteoporosis”.

Bone fractures occur when stress to a bone exceeds the bone’s ability to support that load. In healthy vertebrae, significant stress is required to cause a fracture. But in osteoporotic bones, the threshold for injury is lowered to the point that “compression fractures” may occur with seemingly minimal stress like bending, coughing, or sneezing. A compression fracture causes a wedge-shaped collapse of the front of the vertebral “body”- resembling what would occur after stepping on one edge of an aluminum can.
Compression fractures are two to three times more common in women, and the risk of developing the problem increases over time. People who have had a prior compression fracture are at greater risk for developing a subsequent fracture. Additional risk factors for compression fracture include a family history of osteoporosis, low body weight, recent weight loss, smoking, a sedentary lifestyle, poor dietary choices, inadequate calcium or vitamin D intake, excessive alcohol or caffeine intake, and scoliosis. The American Academy of Orthopedic Surgery recommends bone density screening for osteoporosis in all women over age 65 or post-menopausal women who have suffered a compression fracture. If you have not already done so, you should schedule a bone density screening.
Symptoms of a compression fracture include an “aching” or “stabbing” pain in the back, near the site of fracture. Symptoms can range from minimal to disabling. Often times, pain is referred to the ribs, hip, groin, or buttocks. Be sure to tell your doctor if you have pain or numbness that radiates into your legs, weakness, clumsiness, loss of bowel or bladder control, impotence, fever, unexplained weight loss, night sweats, excessive fatigue, or a history of cancer.
Symptoms from a compression fracture typically lasts for six to 12 weeks. Occasionally, patients will require surgical treatment of a compression fracture, but fortunately, most respond to conservative care. In general, you should maintain a relatively active lifestyle and try to avoid bed rest. If your pain prevents movement, you may talk to your doctor about wearing a brace to limit stress.
Our office will prescribe exercises to help you recover and reduce the risk of subsequent fracture. As your symptoms improve, you can begin incorporating some aerobic exercise, like walking on a treadmill. Studies have shown that light resistance training (i.e. weights and elastic bands) may help you maintain bone density and reduce the risk of future fractures. Supplements to help manage osteoporosis include daily intake of 800-1000 IU of vitamin D and 1000-1200 mg of calcium.
Trigger points in the gluteus minimus
The gluteus minimus is a small but important muscle that lies deep to the gluteus medius. It originates on the gluteal surface of the ilium, and attaches on the greater trochanter of the femur. It’s main actions are to abduct and medically rotate the hip. Trigger points in this muscle refer pain into the buttock and down the lateral and posterior leg, mimicking sciatica. This muscle should be the first to be examined if a straight leg test turns out negative. 
Trigger points in the gluteus medius muscle
The gluteus medius muscle plays an important role in hip and pelvic stability. It originates on the gluteal surface of the ilium, deep to the gluteus Maximus. It inserts on the greater trochanter of the femur. It’s main actions are to abduct the hip and to assist in internal rotation of the hip. It also maintains pelvic stability during walking and running. Trigger points in this muscle will refer pain into the sacrum, the iliac crest, and down the lateral hip and into the thigh. This muscle is often a cause of lower pack pain.
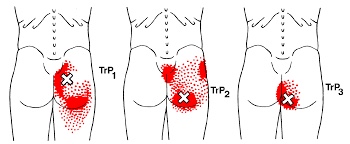
Trigger points in the gluteus Maximus
The gluteus Maximus is the buttock muscle. It originates on the gluteal surface of the ilium, lumbar fascia, sacrum and sacrotuberous ligament. It inserts on the gluteal tuberosity of the femur and the iliotibial tract. Extension and lateral rotation of the hip are it’s main actions. This muscle is heavily involved in activities like ice skating and is a common area to develops trigger points. When trigger points do develop they can refer pain in a crescent pattern from the gluteal fold to the sacrum. Trigger points can also refer pain deep into the buttock itself making it feel like other deeper muscles are involved. These symptoms can sometimes be mistaken for s.i. Joint problems.