Fibromyalgia, although often misdiagnosed and misunderstood, is the second most common musculoskeletal disorder behind osteoarthritis. The condition affects nearly 12 million Americans and is ten times more common in women.
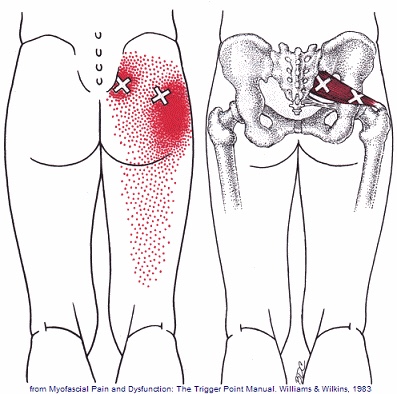
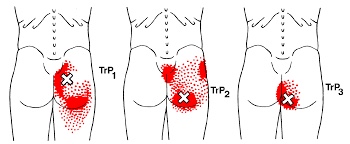
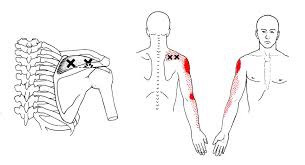
The diagnosis of fibromyalgia is made when a certain set of symptoms has been present for at least three months. The most common symptoms include wide-spread muscle and joint pain, achiness or soreness- especially in the neck, shoulders, back, and hips. Your muscles may constantly feel overworked and tired. Fibromyalgia patients often exhibit a set of predictable “tender points” spread throughout the body. Some patients have trouble sleeping and feel as though they are in a “brain fog” most of the day. This can lead to fatigue or mood changes, like anxiety and depression.

Stress is a known contributor to fibromyalgia, and patients should seek ways to de-stress, including yoga or meditation. Fibromyalgia patients should minimize their caffeine intake, as this is a known stimulant for nervousness, anxiety, and insomnia. Breathing exercises are sometimes helpful.
Although your sleep may be restless, you should try to establish a bedtime routine that gives your body the best chance for recovery. Try to avoid late night electronics, like the television or computer. Keep your bedroom dark, quiet, cool, and distraction-free. Be sure to take time for yourself each day for relaxation or to do something you enjoy. Combat “brain fog” by carrying a notebook or a phone to make notes for important things. Some patients report decreased muscle tightness by applying moist heat or a taking warm bath. The American Pain Society recommends conservative treatment, including chiropractic, along with moderate aerobic exercise.