The lateral pterygoid muscle plays an important role in prober jaw function. It originates on the greater wing of the sphenoid bone and the lateral pterygoid plate, and inserts on the condyloid process of the mandible. It’s action is to pull the head of the mandibular condyle out of the mandibular fossa while opening the jaw. When trigger points develop they refer pain into the temporal mandibular joint and maxillary sinus. This referral is commonly mistaken for TM arthritis. In addition to the referral pain, trigger points in this muscle can also effect proper movement of the jaw.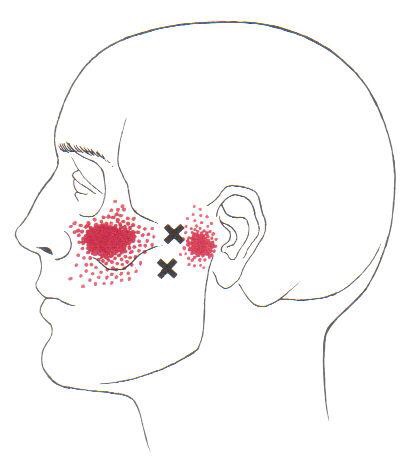

Chronic Pain
FAI starts you on the road to failure.
Your hip socket or “acetabulum” is covered by smooth, glassy cartilage extending all the way to its outer rim. The term “Femoroacetabular impingement” (FAI) means that this rim of cartilage is being pinched when you move your hip into certain positions. Repetitive pinching results in irritation, tearing, or even detachment of this cartilage from your hip socket.

FAI occurs because of a mismatch between the head of your femur and the socket of your hip. The mismatch may be from an abnormally shaped hip bone (cam deformity), or having too much cartilage on the rim of your hip socket (pincer deformity). Most frequently, FAI results from a combination of both (combined or mixed deformity).
FAI is most common in young active people. Although the deformity may be present on both sides, symptoms are usually one-sided. The condition is equally common among men and women. Symptoms of FAI include a constant dull pain with periods of sharp pain, made worse by activity. Walking, pivoting, prolonged sitting, stair climbing, and impact activities like running or jumping can aggravate your symptoms. Snapping, locking, and clicking are common.
Our office will help direct a rehab program to maximize your chance of recovery. You should attempt to stay active, but avoid activities that aggravate symptoms. You may consider temporarily switching to low-impact activities, like stationary biking or water-walking. You should avoid motions that combine flexion and internal rotation, like- getting out of a car with one leg at a time, swimming the breaststroke, or performing squats. Patients with FAI should avoid excessive stretching, as this could aggravate the condition, but will likely benefit from strengthening exercises in the type of treatment provided in this office.
I’ve never baked anything in my life; how do I have a Baker’s Cyst?
Your body has strategically-placed, fluid-filled cushions called “bursa” around each joint. Bursa act to reduce friction where muscular tendons rub on bone. Your knee is surrounded by several bursa that share fluid with the inside of your knee joint and with each other. You can think of this like a chain of lakes connected by streams. If the inside of your knee joint or any of the bursa around your knee becomes inflamed, the entire system fills. When swelling exceeds each individual bursa’s capacity, this fluid creates a soft balloon-like swelling of the popliteal bursa behind your knee called a “Popliteal cyst”, or more commonly a “Baker’s cyst”.
 This swelling is usually not from a problem with the popliteal bursa itself, but rather, inflammation somewhere else in the joint that has distended the popliteal bursa. This swelling is often the result of arthritis or damage to a ligament or cartilage within the knee.
This swelling is usually not from a problem with the popliteal bursa itself, but rather, inflammation somewhere else in the joint that has distended the popliteal bursa. This swelling is often the result of arthritis or damage to a ligament or cartilage within the knee.
A Baker’s cyst is often painful, and the discomfort may increase when you attempt to move your knee. Depending on the severity of your swelling, your symptoms may vary between a feeling of fullness and significant pain. It is not unusual for a Baker’s cyst to change in size from day to day, depending on the amount of swelling. Be sure to tell us if your pain progressively increases when you walk or if you notice warmth, redness or swelling in your calf, as these could be signs of a more significant problem.
Sometimes rest and elevation of your leg help to alleviate pain and swelling. Initially, you may need to avoid activities, like squatting, kneeling, heavy lifting, climbing stairs, or running. Wearing a brace on your knee may compress the cyst and cause an increase in your pain. Since Baker’s cysts are generally a problem that is secondary to another condition, treatment is most effective when directed at the underlying problem.
I’ve got Shin Splints; what do I do?
Shin splints, also called “Medial Tibial Stress Syndrome,” (MTSS) is caused when the muscles of your lower leg pull too hard on your bone, causing local pain and inflammation. Over half of all leg pain in athletes is caused from shin splints. Up to 1/3 of runners and soldiers experience shin splints at some point in their lifetime.
MTSS is an overuse injury frequently seen in sports involving running, jumping, or frequent stopping & starting, i.e. field hockey, soccer and cross-country. Shin splints do not occur overnight but over a period of time, often show up during the first two or three weeks of training for a new season. Shin splints can occur when there are changes to your exercise regimen, such as an increase in activity, change in shoes or a change in the surface you play on. Some doctors refer to these training areas as “the terrible toos,” – too much, too hard, too long, too fast.

Symptoms of shin splints include tenderness or pain over the inside lower portion of your shin. The discomfort begins at the start of exercise and eases as you continue. Some patients report “bumps” when touching the inner portion of their leg bone. Be sure to tell your doctor if you experience weakness, numbness or cold feet during exercise or find a very small area of sensitivity.
Unfortunately, MTSS usually develops during a time when you are training heavily for a sport or an upcoming event. Continuing this activity will often lead to ongoing problems and decreased performance. Shin splints are now believed to be a forerunner to stress fracture, so adequate rest is critical. You may need to consider non-weight bearing cross training, such as using a stationary cycle or pool running.
When directed, your return to activity should start slowly, beginning with a 1/4 mile run and progressing by 1/4 mile each time you have no pain for two consecutive workouts. You should initially avoid running on hard or uneven surfaces and begin at a lower intensity and distance, increasing by no more than 10-15% per week- first increase distance, then pace, and avoid hard or unlevel surfaces, including hills.
Sports creams and home ice massage may provide some relief. Use ice after any activity. Patients who have flat feet are predisposed to developing shin splints and may need arch supports or orthotics. Avoid using heel cushions in your shoes, as they may increase the recurrence of this problem.
Trigger points in the serratus anterior
The serratus anterior muscle is located along the sides of the ribs. It originates on the outer surface of the upper 8-9ribs, and inserts on the medial border of the scapula. This muscle acts on the scapula in several different ways. First it rotates the scapula to turn the glenoid fossa upward. It also protracted and elevates the scapula. And lastly it helps to prevent wining. This muscle is often shortened from prolonged sitting and work on a computer. Active trigger points in this muscle refer pain locally around the trigger point with spillover down the inside of the arm. Pain can also radiate into the inferior angle of the scapula. 
What is my Fibular Head and why does it hurt?
The bone on the outermost portion of your lower leg is called the “fibula.” Your fibula is joined to the larger “tibia” at the ankle and the knee. These connections allow for better function and dispersal of weight (1/6th of your body weight is supported by the fibula).
Proper function of your knee requires natural gliding movements of the tibia/ fibula joint. The diagnosis of “Fibular head dysfunction” means that this joint has been “sprained” or has become “stuck” in an abnormal position. Fibular head problems affect all age groups but are particularly common in young females.

Problems involving the fibular head are often the result of an injury to your leg, hamstring, or ankle. Sports and activities that require violent twisting motions with the knee bent are particularly suspect. Athletes who participate in football, soccer, rugby, wrestling, gymnastics, judo, broad jumping, dancing, long jumping, and skiing may be more likely to suffer this type of injury. Patients who sprain their ankle or slip and fall with their knee flexed under their body may suffer fibular head problems. Sometimes, symptoms begin without an identifiable injury.
Patients with fibular head problems generally complain of pain on the outside of their knee. Symptoms become more intense with weight bearing or when applying pressure over the irritated area. Sometimes, the condition affects both knees at the same time. In more severe cases, you may experience numbness or tingling on the outside of your leg. Be sure to tell your doctor if you notice numbness, tingling, or weakness in your leg or ankle.
In most cases, fibular head dysfunction is treatable with conservative care, like the type provided in our office. Initially, you may need to limit excessive twisting movements and hyperflexion, (i.e. heel to butt.) Taping or bracing may help patients who have suffered a sprain or have an “unstable” joint.
There is nothing great about greater trochanteric pain syndrome. Nothing at all.
Your hip typically has about six small fluid-filled sacs called “bursa” that act as cushions between tendons and bone. One of the most common causes of hip pain is a condition called, “hip bursitis” which means that one or more of your bursas have become painfully inflamed. The broader (more accurate) diagnosis of “Greater trochanteric pain syndrome” (GTPS) describes an uncomfortable collection of problems affecting the outermost portion of your hip. GTPS can include swelling of one or more of the fibrous tendons that attach your muscles onto your hip – a condition called, “tendinitis.” In addition to bursitis & tendonitis, GTPS may originate from tightness in the muscle that travels over your hip en route to your knee- resulting in compression and irritation to your hip.

Greater trochanteric pain syndrome is most common in middle age to elderly adults and is 2-4 times more common in females. Sometimes the problem affects both hips at the same time. Approximately 1/3 of patients with GTPS have lower back pain. Patients who have arthritis in their hips and knees are more likely to suffer from ongoing complaints.
Your symptoms probably include a persistent pain on the outside of your hip, buttock, and upper thigh. Your discomfort may be aggravated by sitting with your leg crossed, arising from a seated position, prolonged standing, climbing stairs, and high-impact activities, like running. Sometimes patients find it difficult to sleep, since lying on the painful hip usually increases symptoms.
For adults, x-rays may or may not be needed to confirm the diagnosis, but children and adolescents usually require films to rule out more serious childhood diseases. Be sure to tell your doctor if you notice that you have a fever, leg numbness, pain radiating significantly beyond your knee, or pain in the front of your groin crease (the area where you leg meets your pelvis.)
Conservative treatment, like the type provided in this office, is successful in about 90% of cases. If you have acute pain, you may need to temporarily limit or discontinue activities that increase your discomfort. Using ice or ice massage at home may help. Some patients find temporarily relief by applying sports creams. Very commonly, patients with pain on the outside of their hip suffer from weakness in one of their buttock muscles, called the “gluteus medius.” When this muscle lacks strength, it is unable to protect your hip during normal activities, like walking. Research has shown that strengthening your hip has a dramatic effect on your progress.
Athletes should avoid running on a banked surface, like the crown of a road or indoor track. Be sure to reverse directions each mile if you run on a circular track. Avoid running on wet or icy surfaces, as this can cause increased tension in your hip. Runners with a “lazy” narrow-based running gait will benefit by increasing their step width to minimize stress on their hip. Cyclists need to make sure that their seat is not positioned too high. Overweight patients should consider weight reduction programs.
Pes Anserine Bursitis; What Is It?
The term “pes anserine” is Latin for goose’s foot, and describes the appearance of three tendons that converge and insert on the inner portion of your knee. The pes anserine bursa is a fluid-filled, friction-reducing cushion, sandwiched between these tendons and your leg bone.
Injuries or irritation can cause the lining of the bursa to produce too much fluid, resulting in painful swelling. Patients with knee osteoarthritis are likely to have chronic irritation of the pes anserine bursa. The condition is more common in overweight patients, diabetics, and females. Runners and athletes in sports that require rapid side-to-side movements (i.e. football, soccer, tennis, etc.) are more likely suffer from the condition. Swimmers who do the breast stroke commonly suffer from pes anserine bursitis.
 Symptoms include pain on the inner side of your knee, just below the joint. Your pain is probably worse when you stand up or walk stairs. Discomfort increases during activities that require side-to-side movements (i.e. tennis, dancing). Be sure to tell your doctor if you notice clicking, popping, or locking of your knee, excessive thirst, excessive urination, fever, or pain & swelling in your calf.
Symptoms include pain on the inner side of your knee, just below the joint. Your pain is probably worse when you stand up or walk stairs. Discomfort increases during activities that require side-to-side movements (i.e. tennis, dancing). Be sure to tell your doctor if you notice clicking, popping, or locking of your knee, excessive thirst, excessive urination, fever, or pain & swelling in your calf.
In addition to the treatment provided by our office, you may find relief by applying home ice or ice massage for 8-10 minutes. Having flat feet places additional stress on the inside of your knee, so patients with fallen arches will benefit from arch supports or orthotics. Overweight patients will benefit from a diet and exercise program.
Trigger points in the iliopsoas muscle
This muscle originates on the bodies and disks of T12-L5 and the inner ilium. It inserts on the lesser trochanter of the femur. The psoas flexes the hip when the spine is fixed. When the leg is fixed it extends the lumbar spine increasing lumbar lordosis. This Muscle is often chronically shortened due to inactivity and sitting posture. When trigger points are present they will refer pain primarily to the lower lumbar area and the sacrum as well as into the anterior thigh. Trigger points in the iliopsoas muscle can mimic appendicitis.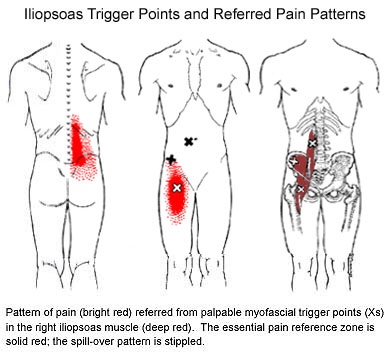
My abductors are weak, what does that mean?
One very important job of your hip muscles is to maintain the alignment of your leg when you move. One of the primary hip muscles, the gluteus medius, plays an especially important stabilizing role when you walk, run, or squat. The gluteus medius attaches your thigh bone to the crest of your hip. When you lift your left leg, your right gluteus medius must contract in order to keep your body from tipping toward the left. And when you are standing on a bent leg, your gluteus medius prevents that knee from diving into a “knock knee” or “valgus” position. 
Weakness of the gluteus medius allows your pelvis to drop and your knee to dive inward when you walk or run. This places tremendous strain on your hip and knee and may cause other problems too. When your knee dives inward, your kneecap is forced outward, causing it to rub harder against your thigh bone- creating a painful irritation and eventually arthritis. Walking and running with a relative “knock knee” position places tremendous stress on the ligaments around your knee and is a known cause of “sprains”. Downstream, a “knock knee” position puts additional stress on the arch of your foot, leading to other painful problems, like plantar fasciitis. Upstream, weak hips allow your pelvis to roll forward which forces your spine into a “sway back” posture. This is a known cause of lower back pain. Hip muscle weakness seems to be more common in females, especially athletes.
Weakness of the gluteus medius allows your pelvis to drop and your knee to dive inward when you walk or run. This places tremendous strain on your hip and knee and may cause other problems too. When your knee dives inward, your kneecap is forced outward, causing it to rub harder against your thigh bone- creating a painful irritation and eventually arthritis. Walking and running with a relative “knock knee” position places tremendous stress on the ligaments around your knee and is a known cause of “sprains”. Downstream, a “knock knee” position puts additional stress on the arch of your foot, leading to other painful problems, like plantar fasciitis. Upstream, weak hips allow your pelvis to roll forward which forces your spine into a “sway back” posture. This is a known cause of lower back pain. Hip muscle weakness seems to be more common in females, especially athletes.
You should avoid activities that cause prolonged stretching of the hip abductors, like “hanging on one hip” while standing, sitting crossed legged, and sleeping in a side-lying position with your top knee flexed and touching the bed. Patients with fallen arches may benefit from arch supports or orthotics. Obesity causes more stress to the hip muscles, so overweight patients may benefit from a diet and exercise program. The most important treatment for hip abductor weakness is strength training. Hip strengthening is directly linked to symptom improvement. Moreover, people with stronger hip muscles are less likely to become injured in the first place. The exercises listed below are critical for your recovery.
Meet the Hip Cycle. You can thank me later.
1. Side lying with back and shoulders against a wall so you can’t roll back.
2. Bend your bottom leg and put the sole of your foot against the wall to be more stable.
3. Start position is with your foot directly in line with your hip. Do not let it get any lower than that. The highest point of your foot needs to be the bump on the outside of your ankle.
Do 5-10 reps of each of the following without rest between exercises twice a day. The goal is 20 reps each.
a. 6″ leg raises in abduction
b. Knee up to chest (90* knee and hip)
c. 12″ leg raises into abduction
d. Bicycling (knee up to chest, extend knee and sweep back to start with leg straight)
e. Clockwise circles
f. Counterclockwise circles
Good luck.
