The supraspinatus is a muscle of the rotator cuff. Is sits above the infraspinatus and originates on the supraspinous fossa of the scapula. It’s insertion point is the superior facet of the greater tubercle of the humerus. It’s main function is to abduct the arm at the glenohumeral joint working with the deltoid. All rotator cuff muscles act to secure and support the head of the humerus in the glenoid fossa during arm movements acting as a sling. This muscle often gets impinged during overhead movements such as painting a ceiling. When trigger points form in this muscle they primarily refer a deep achy pain into the mid deltoid area with spillover pain radiating down the arm into the elbow.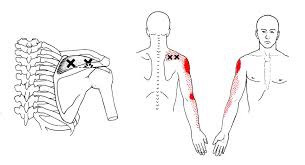
Chiropractic
Can Chiro help me?

Chiropractic is the most widely accepted and most frequently used type of “alternative” healthcare in the United States. This is largely due to the fact that it works, and because of that, there has been a steady increase in acceptance by the public, third-party payers, and the Federal government. Since the mid-1990s, a number of outside (non-chiropractic) observers have suggested that chiropractic has now entered mainstream healthcare.
One can position chiropractic as being BOTH alternative and mainstream. It is “alternative” since it approaches healthcare from an entirely different direction compared to the primary care medical profession. Chiropractic is non-surgical and promotes diet and nutritional approaches vs. drugs and surgery. Chiropractic is also arguably “mainstream” as it has evolved into a strongly utilized form of primary care through popular acceptance and utilization by the public.
So, what role does chiropractic play in today’s health delivery system? This question is still being debated, but there appears to be three camps: 1) Specialist—limited to musculoskeletal (MSK) complaints on an interdisciplinary primary healthcare team; 2) Primary healthcare “gatekeepers” that focus on ambulatory MSK complaints; 3) Generalist primary healthcare provider of “alternative or complementary” medicine that manage and/or co-manage both MSK AND non-MSK conditions.
Looking at this from the patient or “consumer” perspective, chiropractic already plays an important role in the healthcare delivery for many patients. In 1993, a report claimed 7% of American adults had received chiropractic care during the prior year. According to a 2015 Gallup poll (that included 5,442 adults, aged 18+, surveyed between 2/16/15 and 5/6/15) entitled, Majority in U.S. Say Chiropractic Works for Neck, Back Pain, “Chiropractic care has a positive reputation among many US adults for effective treatment of neck and back pain, with about six in 10 adults either strongly agreeing (23%) or agreeing somewhat (38%) that chiropractors are effective at treating these types of pain.”
The “highlights” from this Gallup poll include: 1) Two-thirds say chiropractic is effective for neck and back pain. 2) Many adults say chiropractors think of the patient’s best interest. 3) More than 33 million adults in the United States (US) saw a chiropractor in the twelve months before the survey was conducted. That means roughly 14% of U.S. adults saw a chiropractor in the 12 months prior to the survey (vs. 7% in 1993). An additional 12% who responded to the Gallup pollsters saw a chiropractor in the last five years but not in the last 12 months. Overall, 51% of those polled had previously seen a chiropractor.
Whether or not you have personally utilized chiropractic, the educational process, licensing requirements, public interest, third-party payer systems, and interprofessional cooperation ALL support firm ground for which you can comfortably and confidently seek chiropractic care for your complaints.
We realize you have a choice in whom you consider for your health care provision and we sincerely appreciate your trust in choosing our service for those needs. If you, a friend, or family member requires care, we would be honored to render our services.
My ankle hurts…….
The posterior tibialis muscle begins deep in your calf. The muscle is connected to the arch of your foot by a tendon that runs along the inside of your ankle, just behind the large bump called the medial malleolus. When you walk, the posterior tibialis muscle lifts the arch of your foot. 
Posterior tibial tendon dysfunction is one of the most common foot and ankle problems. The tendon may be damaged from an acute injury, like an accident or fall. More commonly, problems arise from overuse or repeated strain. Ongoing irritation slowly damages the tendon’s fibers and eventually leads to weakening and degeneration. This decreases the tendon’s ability to support your foot when you walk. As the tendon becomes less effective, the arch of your foot is allowed to collapse, which further increases the strain on the muscle and tendon.
The condition is often triggered from overuse and/or training on excessively hard surfaces. Other factors that can contribute to posterior tibial tendon dysfunction include: obesity, diabetes, hypertension, prior surgery or steroid injections.
Symptoms include pain or swelling along the course of the tendon, particularly behind your inner ankle bone. Symptoms often begin following an increase in training intensity or duration. Standing, walking, or running will likely increase your discomfort. Your pain may be aggravated by spending prolonged periods of time on your feet, especially, when standing tiptoe and walking stairs or uneven surfaces.
Early diagnosis and treatment is important to slow progression of the disorder. You may need to temporarily limit weight-bearing activity to allow your tendon to heal. Using a stationary cycle, elliptical machine, or swimming can be good alternatives to walking and running. Your doctor will likely prescribe arch supports or orthotics to help support your foot. You will be given exercises to strengthen the posterior tibialis muscle. These exercises should be performed while wearing shoes with good arch supports. In certain instances, a walking cast or boot may be needed to temporarily protect your foot.
The Dreaded Lateral Ankle Sprain
“Ligaments” are made up of many individual fibers running parallel to each other and bundled to form a strong fibrous band. These fibrous bands hold your bones together. Just like a rope, when a ligament is stretched too far, it begins to fray or tear. “Sprain” is the term used to describe this tearing of ligament fibers.
Sprains are graded by the severity of damage to the ligament fibers. A Grade 1 sprain means the ligament has been painfully stretched, but no fibers have been torn. A Grade 2 sprain means some, but not all, of the ligaments’ fibers have been torn. A Grade 3 sprain means all of the ligaments’ fibers have been torn, and the ligament no longer has the ability to protect the joint.


Ankle sprains are the most common soft-tissue injury and will affect up to 20% of active people at some point in their life. Most ankle sprains occur because you have “rolled your ankle” inward. Sprains on the outer side of your ankle are much more common than sprains on the inner side. People who have suffered a prior ankle injury are more likely to suffer subsequent ankle injuries.
Ankle sprains cause pain and swelling over the outside of your ankle. Walking may be difficult, and bruising is common. Be sure to tell your doctor if you experience numbness, tingling, or a dramatic cold sensation in your foot, as this may indicate more significant injury.
Ankle sprains can be successfully managed but will require some work on your part. You can help reduce swelling by elevating your ankle by lying or sitting with your foot elevated or by using an ACE wrap for compression. Applying ice or ice massage for 10 minutes each hour may help relieve swelling. Depending upon the severity of your sprain, you may need to wear an ankle brace to help protect you from further injury. If walking is painful, crutches may be necessary.
Initially, a period of rest may be necessary in order to help you heal. Mild Grade 1 sprains may allow return to sport in a couple of days, while more severe injuries may take six weeks or longer to recover. Surgery is rarely necessary.
Where should you turn when back pain strikes?

Where should you turn when back pain strikes?
https://tribunecontentagency.com/article/where-to-turn-for-low-back-pain-relief/
Chiropractic should be a first line defence when back pain strikes. We are special trained to recognize the cause of back pain and treat when appropriate. When the cause is outside the scope of our practice, we are able to educate you on where you should go next.
Is there an actual cure all?

No; but exercise seems to be as close as we will ever get!
Some of you may have heard about how a modified form of boxing is helping patients with Parkinson’s disease (PD). If you haven’t, it’s been observed that people with Parkinson’s disease (PD) who engage in this boxing-like exercise routine can enhance their quality of life and even build impressive gains in posture, strength, flexibility, and speed. Proponents of the program report that regardless the degree of severity of PD, participants have a happier, healthier, and higher quality of life.
But must it be boxing? Maybe not. A report presented at the International Congress of Parkinson’s Disease and Movement Disorders in San Diego in June 2015 found that patients with Parkinson’s disease who began regular exercise early into the PD process had a much slower decline in their quality of life when compared with those who started exercising later. The researchers found just 2.5 hours per week of exercise is needed to improve quality of life scores. According to the report, it didn’t matter what exercise the participants did — simply getting up and moving for a total of 2.5 hours/week was reportedly enough (that’s only 20-25 minutes / day)!
Looking beyond Parkinson’s, other chronic conditions also benefit from adding exercise into a person’s lifestyle. Studies show that regular exercise as simple as walking helps reduce one’s risk for memory loss, and it slows down functional decline in the elderly. Incorporating aerobic exercise into one’s lifestyle can also improve reaction time in people at ALL AGES. Exercise has also been shown to improve both physical and emotional well-being in those afflicted with Alzheimer’s disease with as little as 60 minutes/week of moderate exercise! Patients with multiple sclerosis (MS) have also reported less stiffness and less muscle wasting when using exercise machines, aquatic exercise, and/or walking.
Research has shown just 30 minutes of brisk exercise three times a week can help reduce depressive symptoms in patients with mild-to-moderate depression. In a study involving teenagers, those who engaged in sports reported a greater level of well-being than their sedentary peers, and the more vigorous the exercise, the better their emotion health! In kids 8-12 years old, physical inactivity is strongly linked to depression.
Even anxiety, stress, and depression associated with menopause are less severe in those who exercise! So LET’S ALL GET OUT THERE AND EXERCISE!!!
What is Scoliosis?

Your spine is made up of 24 bones that stack on top of each other- normally in a straight line. “Scoliosis” means that your spine is curving from side to side, rather than being straight. Scoliosis affects between 1-3% of the population. Scoliosis may begin at any time between birth and adulthood but is most common during times that your skeleton is growing rapidly. Most cases of scoliosis begin between the ages of 13 and 18. Researchers are not completely certain why some people develop scoliosis, but they have found that the problem tends to run in families.
The curve of your scoliosis may be measured with an x-ray. Although some curves get worse, most do not. In fact, only ¼ of all adolescent idiopathic scoliosis curves will progress. Small curves in mature patients have a low risk of progression (2%), while large curves in younger patients progress more frequently. (70%) Curve progression is more common in girls, especially those with larger curves (greater than 20 degrees). Your doctor may need to monitor your scoliosis for progression by performing x-rays every 6-18 months.
Scoliosis may cause your shoulders, hips, or waist to be unlevel. Most curves are classified as “right thoracic”, which means that the peak of your curve protrudes toward the right. This is often accompanied by a forward rotation of your right shoulder and “winging” of your right shoulder blade. Many patients have a secondary curve in their lower spine that helps to balance their body. The majority of patients with mild to moderate scoliosis have no symptoms, but approximately ¼ report back pain. Unfortunately, scoliosis increases your risk of developing back pain later in life.
The primary goal of treatment is to stop curve progression. While many cases can be slowed or even reversed through appropriate management, it is important to recognize that others may progress in spite of the best care. Conservative care, including spinal manipulation (like the type provided in our office) has been shown to help some patients with scoliosis. Exercise is another effective treatment for scoliosis. It is important that you clearly understand your home exercise program and that you perform it consistently.
Patients with larger curves (30-40 degrees), or those who are at high risk for progression may benefit from wearing a brace. Braces have been shown to decrease the need for surgery in about three out of four patients. Fortunately, less than 0.3% of all scoliosis cases will ever require surgery.
You should avoid carrying heavy back packs and consider switching to a wheeled version, if necessary. Sports and exercise will not worsen most cases of scoliosis, and you should continue to participate in the things you enjoy unless directed otherwise by your doctor. The diagnosis of scoliosis is always discouraging, but you must focus on what it is really most important. Be confident in who you are! Don’t let something like a curved spine (or any other medical condition) define you as a person.
Hip Abductor Weakness

One very important job of your hip muscles is to maintain the alignment of your leg when you move. One of the primary hip muscles, the gluteus medius, plays an especially important stabilizing role when you walk, run, or squat. The gluteus medius attaches your thigh bone to the crest of your hip. When you lift your left leg, your right gluteus medius must contract in order to keep your body from tipping toward the left. And when you are standing on a bent leg, your gluteus medius prevents that knee from diving into a “knock knee” or “valgus” position.
Weakness of the gluteus medius allows your pelvis to drop and your knee to dive inward when you walk or run. This places tremendous strain on your hip and knee and may cause other problems too. When your knee dives inward, your kneecap is forced outward, causing it to rub harder against your thigh bone- creating a painful irritation and eventually arthritis. Walking and running with a relative “knock knee” position places tremendous stress on the ligaments around your knee and is a known cause of “sprains”. Downstream, a “knock knee” position puts additional stress on the arch of your foot, leading to other painful problems, like plantar fasciitis. Upstream, weak hips allow your pelvis to roll forward which forces your spine into a “sway back” posture. This is a known cause of lower back pain. Hip muscle weakness seems to be more common in females, especially athletes.
You should avoid activities that cause prolonged stretching of the hip abductors, like “hanging on one hip” while standing, sitting crossed legged, and sleeping in a side-lying position with your top knee flexed and touching the bed. Patients with fallen arches may benefit from arch supports or orthotics. Obesity causes more stress to the hip muscles, so overweight patients may benefit from a diet and exercise program. The most important treatment for hip abductor weakness is strength training. Hip strengthening is directly linked to symptom improvement. Moreover, people with stronger hip muscles are less likely to become injured in the first place.
Trigger points in the triceps muscle.
The tricep muscle is named for its three heads long, medial, and lateral. The long head originates on the infraglenoid tubercle, the medial head on the posterior humerus, and the lateral head on the posterior humerus as well. They join together to insert on the Olecranon process of the ulna. The triceps function to extend the elbow. Strong extension under resistance can cause trigger points to form. Pain referred from triceps trigger points can be felt in the posterior shoulder and down the posterior forearm, as well as in in the olecranon process and the lateral epicondyle which can cause “tennis elbow” pain.
My knee hurts; I must have bad knees….

Due to bipedal locomotion (walking around on two legs), foot and ankle problems have the potential to affect EVERYTHING above the feet—even the knees!
When analyzing the way we walk (also known as our gait), we find when the heel strike takes place, the heel and foot motion causes “supination” or the rolling OUT of the ankle. As the unloaded leg begins to swing forwards, there is a quick transition to pronation where the heel and ankle roll inwards and the medial longitudinal arch (MLA) of the foot flattens and pronates NORMALLY!
During the transition from supination to pronation, the flattening of the MLA acts like a spring to propel us forwards followed by the “toe off”, the last phase, as we push off with our big toe and the cycle starts with the other leg. However, if you watch people walk from behind, you will see MANY ankles roll inwards too much. This is call “hyperpronation” and that is NOT NORMAL!
So at what point does this normal pronation become hyperpronation? The answer is NOT black and white, as there is no specific “cut-off” point but rather, a range of abnormal. Hence, we use the terms mild, moderate, and severe hyperpronation to describe the variance or the degrees of abnormality. Hyperpronation can lead to the development of bunions and foot/ankle instability that can cause and/or contribute to knee, hip, pelvis, and spinal problems—even neck and head complaints can result (the “domino effect”)!
One study looked at the incidence of hyperpronation in 50 subjects who had an anterior cruciate ligament (ACL) rupture vs. 50 without a history of knee / ACL injury. They found the ACL-injured subjects had greater pronation than the noninjured subjects suggesting that the presence of hyperpronation increases the risk of ACL injury.
Doctors of chiropractic are trained to evaluate and treat knee conditions of all kinds. Often this may include prescribing exercises or utilizing foot orthotics in an effort to restore the biomechanics of the foot, which can have positive effects not only on the knees but also further up the body.
