Dr Janet travel coined the term trigger point in 1942 to describe clinical findings with characteristics of pain related a discrete irritable point in muscle or fascia that was not caused by acute trauma, inflammation, degeneration, neoplasm or infection. The painful point can be palpated as a nodule or tight band in the muscle that can produce a local twitch response when stimulated. Palpation of the trigger point reproduces the pain and symptoms of the patient and the pain radiates in a predictable referral pattern specific to the muscle harbouring the trigger point.
Arthritis
Snapping Hip. Not as horrific as it sounds.
The muscle responsible for flexing your hip toward your trunk, is called the Psoas. This muscle begins on your lower spine and passes through your pelvis to attach onto the top of your femur (thigh bone). Along this course, the muscle travels across the front of your hip socket and over several bony prominences. If the muscle is too tight, its tendon may rub over these “bumps”. This occasionally produces an audible snapping sound, hence the moniker, “snapping hip”, aka “psoas tendinopathy”.
 The tendon can be irritated by an acute injury, but more commonly from overuse- particularly repeatedly flexing your hip toward your trunk. The condition is also known as “dancer’s hip” or “jumper’s hip”, as movements associated with these activities are known culprits. Likewise, the condition is frequently seen in athletes who participate in rowing, track and field, hurdling, running (especially uphill), soccer, and gymnastics.
The tendon can be irritated by an acute injury, but more commonly from overuse- particularly repeatedly flexing your hip toward your trunk. The condition is also known as “dancer’s hip” or “jumper’s hip”, as movements associated with these activities are known culprits. Likewise, the condition is frequently seen in athletes who participate in rowing, track and field, hurdling, running (especially uphill), soccer, and gymnastics.
Your symptoms may include a “snapping” sound or sensation when you flex and extend your hip- although many cases are silent. Repeated rubbing causes inflammation and subsequent deep groin pain that can radiate to the front of your hip or thigh. Long-standing problems can trigger weakness or even limping.
The diagnosis of snapping hip is frequently overlooked. In fact, some studies show that identification is often delayed more than two years, while other potential causes are pursued. Fortunately, your problem has been recognized, and our office has several treatments to help you recover.
Psoas problems often start when one group of muscles is too tight, while another is too loose. Your home exercises will help to correct this problem. Depending upon the severity of your condition, you may need to avoid certain activities for a while. You should especially avoid repetitive hip flexion. Prolonged seated positions can encourage shortening of your hip flexors so be sure to take frequent breaks. Patients with fallen arches may benefit from arch supports.
What to expect with a trigger point massage.
A treatment with Bryan is very user friendly. And, no, you don’t have to remove any clothing. However, bringing a t-shirt and a pair of shorts or sweats is recommended.

The first time you come for a treatment you will be asked to fill out a Client History form. Bryan will go over the information you provide, asking for more detail and discussing the type of pain you are having and its location.
The treatment itself involves locating the Trigger Points in the muscle or soft tissue and applying a deep focused pressure to the Point. This will reproduce the pain and the referral pattern that is characteristic of that pain.
The treatment will be uncomfortable at first, but as the Trigger Points release, the pain will decrease. The pressure will always be adjusted to your tolerance level. If, at any time, you feel too uncomfortable you can ask Bryan to ease off a bit.
Depending on your specific problem, Bryan may also use some stretching and / or range-of-motion techniques, as needed.
After treatment, it is usually recommended that the client apply moist heat to the area treated.
Lumbar Spine Stabilization

This is a great way to increase the stability of your lower back.
- Lie with your stomach over a therapeutic ball while stabilizing yourself with your feet and arms and keep your head in line with your body.
- Tighten your abdominal muscles to flatten the spine by pulling your belly button towards your back and hold the contraction throughout the exercise.
- Bend one knee and lift it up towards the ceiling.
- Lower the leg and repeat on the other side.
Hip Abductor Weakness

* The gluteus medius contributes approximately 70% of the abduction force required to maintain pelvic leveling during single leg stance.
* Hip abductor strength is the single greatest contributor to lower extremity frontal plain alignment during activity.
* There is no “typical” presentation for hip abductor weakness, but the problem must be considered in any patient with lower chain symptomatology, particularly those with hip tendinopathy, greater trochanteric pain syndrome, iliotibial band syndrome, patellofemoral pain syndrome, ACL injury, medial knee pain, and lower back pain.
*Hip abductor weakness is often accompanied by lower crossed syndrome – a larger pattern of biomechanical dysfunction involving weakness of the abdominal wall and hypertonicity in the hip flexors and paraspinal musculature. Evaluation should include a relatively global assessment of lumbopelvic muscle and joint function. Additionally, clinicians should assess for the presence of foot hyperpronation in patients with hip abductor weakness.
Referenced from:
ChiroUp.com “Hip Abductor Weakness Clinical Pearls
Workstation Ergonomics
Ergonomics is the science of adjusting your workstation to minimize strain in the following ways:
✓ Maintain proper body position and alignment while sitting at your desk – Hips, knees and elbows at 90 degrees, shoulders relaxed, feet flat on floor or footrest.
✓ Wrists should not be bent while at the keyboard. Forearms and wrists should not be leaning on a hard edge.
✓ Use audio equipment that keeps you from bending your neck (i.e., Bluetooth, speakerphones, headsets).
✓ Monitors should be visible without leaning or straining and the top line of type should be 15 degrees below eye level.
✓ Use a lumber roll for lower back support.
✓ Avoid sitting on anything that would create an imbalance or uneven pressure (like your wallet).
✓ Take a 10-second break every 20 minutes: Micro activities include: standing, walking, or moving your head in a “plus sign” fashion.
✓ Periodically, perform the “Brugger relief position” (See video below) -Position your body at the chair’s edge, feet pointed outward. Weight should be on your legs and your abdomen should be relaxed. Tilt your pelvis forward, lift your sternum, arch your back, drop your arms, and roll out your palms while squeezing your shoulders together. Take a few deep cleansing breaths.
Can Adjustments Help Relieve Neck Pain?
There have been MANY studies conducted on the benefits and efficacy of spinal manipulation to treat back pain—so much so that many medical doctors frequently refer patients with back pain to chiropractors for this service. But what about neck pain?
Although it’s taken a little longer to compile the evidence, there is now substantial research to support that spinal manipulation for neck pain is equally effective as it is for low back pain in regards to improving pain levels, function, and quality of life.
Multiple reviews and meta-analyses (studies that evaluate the research over a series of years) indicate that mobilization, manipulation, and exercise all work alone but appear to give the best long-term benefits when used in combination with each other.
In the acute and subacute stages of neck pain, studies show cervical manipulation is more effective than various combinations of analgesics, muscle relaxants, and nonsteroidal anti-inflammatory drugs (NSAIDs) for improving pain and function in both the short and intermediate term.
Studies show that thoracic or mid-back manipulation is also very helpful for patients with neck pain. Chiropractic approaches often include a combination of spinal manipulation, manual cervical traction, figure-8 mobilization, and deep tissue trigger point/active release forms of therapy.
As noted above, the inclusion of exercise yields the best long-term benefits, especially for chronic neck pain.
One such exercise is Cranio-cervical flexion (deep neck flexor strengthening): Tuck the chin inwards, pushing the mid part of the neck backward with or without resisting into your fingers/hands or a towel wrapped around the neck. A gradual crescendo of pressure followed by a gradual release (or decrescendo) works well!
Another great exercise is Fiber Stretching: Side-bend the head and neck while applying gentle over-pressure while simultaneously reaching downward with the opposite arm/hand, searching for tight muscle fibers. Try combining forward and backward rotations and chin glide head movements while applying the over-pressure/reach combinations, and work each tight fiber until it loosens up.
There are many other exercises your doctor of chiropractic can show you, but these are a great start!
What is Cervical Spondylosis?
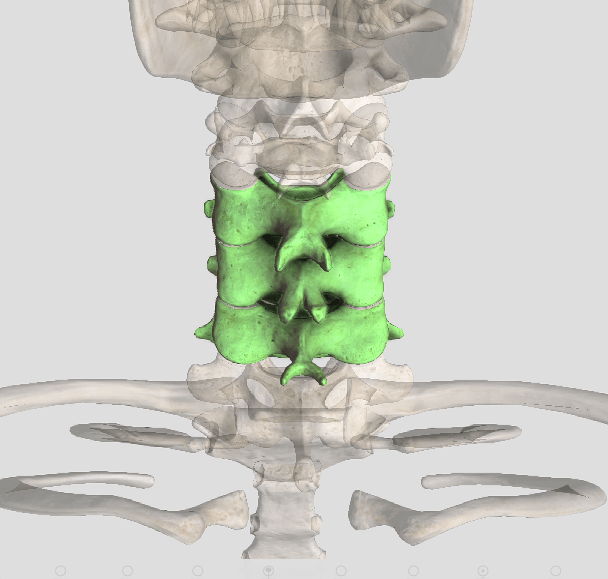
Cervical spondylosis (CS) is another term for osteoarthritis (OA) of the neck. It is a common, age-related condition that you will probably develop if you live long enough. Or, if you suffered a neck injury as a youth, it can develop within five to ten years of the injury, depending on the severity. According to the Mayo Clinic, CS or OA affects more than 85% of people over 60 years old, and that is probably a conservative estimate!
Common symptoms associated with CS/OA vary widely from no symptoms whatsoever to debilitating pain and stiffness. For example, when CS crowds the holes through which the nerves and/or spinal cord travel, it creates a condition called spinal stenosis that can result in numbness, tingling, and/or weakness. In severe cases, this can even affect bowel or bladder control (which is an EMERGENCY)!
CS occurs when the normal slippery, shiny cartilage surfaces of the joint(s) gradually thin and eventually wear away. Bone spurs often form, which results from the body trying to stabilize an unstable joint. In some cases, the spurs can actually fuse a joint, which often helps reduce pain. (Bone spurs can also form if the intervertebral disks or shock-absorbing pads between the vertebrae are injured or become dehydrated due to arthritic conditions.)
Risk factors associated with CS include: aging, injury, years of heavy lift/carry job demands, and jobs and/or hobbies that require the neck to be outside of a neutral position (like years of pinching a phone between the ear and shoulder). Genetics and bad habits (like smoking) also play a role in CS. Obesity and inactivity also worsens the severity of CS symptoms.
The good news is that even though most of us will have CS, it is usually NOT a disabling condition. However, CS may interfere with our normal activities. Depending on its location, pain may feel worse in certain positions, like when sneezing or coughing or with movements like rotation or looking upwards.
Stiffness is a common symptom, which can vary with weather changes. Too little as well as too much activity can be a problem, but the BEST way to self-manage CS is to keep active! Range of motion exercises, strength training, and walking all help reduce the symptoms of CS.
Doctors of chiropractic are trained to identify CS/OA. Gentle manipulation, mobilization, nutritional counseling, exercise training, modalities (and more) can REALLY HELP!
Why Crack?

We all know what it’s like to have neck pain—whether it’s after a long drive, pinching the phone between the head and shoulder, star-gazing, or from talking to someone who is seated off to the side. There are many causes of neck pain, but the question of the month is, how do chiropractic adjustments help neck pain? Let’s take a look!
Chiropractic, when broken down into its fundamental Greek derivatives, means “hand” (cheir) and “action” (praxis). The technique most often associated with chiropractic is spinal manipulation where a “high velocity, low amplitude” thrust is applied to specific vertebrae in the spine, which does several things: 1) It restores mobility in an area with restricted movement; 2) It stimulates the sensory “neuroreceptors” in joint capsules, which has a muscle relaxing reflex effect; 3) It can affect surrounding neurological structures in certain parts of the spine such as the parasympathetic (cranial & sacral regions) and sympathetic (mid-back) nervous systems, which can have beneficial effects on the digestive system, cardiovascular system, and other body systems not typically thought about when seeking chiropractic care.
Joint manipulation is not new, as it can be traced back to as early as 400 BCE. The profession of chiropractic began in the later 1800s and has grown in popularity ever since. There is now an overwhelming body of evidence that supports spinal manipulation as both a safe and highly effective treatment for neck and back pain, headaches, and many other maladies.
It’s important to note that there are many different types of manual therapies that chiropractors utilize when caring for neck pain patients. There are “low-velocity, low amplitude” or non-thrust techniques that do NOT produce the “crack” that is frequently associated with chiropractic adjustments. The term “mobilization” is often used when referencing these non-thrust methods, and this often incorporates a combination of manual traction (pulling of the neck), left to right and front to back “gliding” movements usually starting lightly and gradually increasing the pressure as tolerated. In many cases, a doctor of chiropractic may utilize a combination of manipulation and mobilization as well as “trigger point therapy” (applying sustained pressure over tight “knots” in muscles), depending on a patient’s needs.
Meds or Chiro first?

Although both medication and chiropractic are utilized by neck pain sufferers, not everyone wants to or can take certain medications due to unwanted side effects. For those who aren’t sure what to do, wouldn’t it be nice if research was available that could answer the question posted above? Let’s take a look!
When people have neck pain, they have options as to where they can go for care. Many seek treatment from their primary care physician (PCP). The PCP’s approach to neck pain management usually results in a prescription that may include an anti-inflammatory drug (like ibuprofen or Naproxen), a muscle relaxant (like Flexeril / cyclobenzaprine), and/or a pain pill (like hydrocodone / Vicodin). The choice of which medication a PCP recommends hinges on the patient’s presentation, patient preference (driven from advertisements or prior experiences), and/or the PCP’s own preference.
Although it’s becoming increasingly common to have a PCP refer a neck pain patient for chiropractic care, this still does not happen for all neck pain patients in spite of strong research supporting the significant benefits of spinal manipulation to treat neck pain. One such study compared spinal manipulation, acupuncture, and anti-inflammatory medication with the objective of assessing the long-term benefits (at one year) of these three approaches in patients with chronic (>13 weeks) neck pain. The study randomly divided 115 patients into one of three groups that were all treated for nine weeks. Comparison at the one-year point showed that ONLY those who received spinal manipulation had maintained long-term benefits based on a review of seven main outcome measures. The study concludes that for patients with chronic neck pain, spinal manipulation was the ONLY treatment that maintained a significant long-term (one-year) benefit after nine weeks of treatment!
In a 2012 study published in medical journal The Annals of Internal Medicine, 272 acute or sub-acute neck pain patients received one of three treatment approaches: medication, exercise with advice from a health care practitioner, or chiropractic care. Participants were treated for twelve weeks, with outcomes assessed at 2, 4, 8, 12, 26, and 52 weeks. The patients in the chiropractic care and exercise groups significantly outperformed the medication group at the 26-week point AND had more than DOUBLE the likelihood of complete neck pain relief. However, at the one-year point, ONLY the chiropractic group continued to demonstrate long-term benefits! The significant benefits achieved from both exercise and chiropractic treatments when compared with medication make sense as both address the cause of neck pain as opposed to only masking the symptoms.
With results of these studies showing acute, subacute, as well as chronic neck pain responding BEST to chiropractic care, it only makes sense to TRY THIS FIRST!
