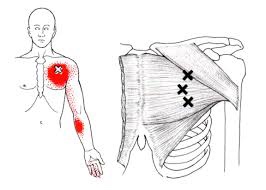
The pectoralis major or “pecs” is commonly thought of as the chest muscle. It originates on the clavicle, sternum, costal cartilage , and the external oblique aponeurosis. It inserts on the intertubercular groove of the humerus. Its main actions are to adduct the shoulder and to internally rotate the humerus. This muscle gets chronically shortened by a rounded shoulder forward posture such as from prolonged sitting. Tightness in this muscle can cause strain in the rhomboids and traps. When trigger points form in this muscle they refer pain into the anterior shoulder, as well as the anterior chest and medial aspect of the arm. Trigger points in the pecs can also cause nipple hypersensitivity. Trigger points in the left pec muscle can mimic heart pain.
Arm Pain
Feels just like Carpal Tunnel but isn’t Carpal Tunnel……
Your Median Nerve begins in your neck and travels down your arm on its way to your hand. This nerve is responsible for sensation on the palm side of your first 3 ½ fingers and also controls some of the muscles that flex your fingers. The median nerve can sometimes become entrapped near your elbow as it travels through a muscle called the “pronator teres”. Compression of the median nerve by the pronator muscle is called “Pronator Syndrome.”

Pronator syndrome is often brought on by prolonged or repeated wrist and finger movements, i.e., gripping with the palm down. Carpenters, mechanics, assembly line workers, tennis players, rowers, and weight lifters are predisposed to this problem. The condition is more common in people with excessively developed forearm muscles and is also more common in your dominant arm. Pronator syndrome most often affects adults age 45-60 and females are affected about four times more frequently than males. People who suffer from diabetes, thyroid disease, and alcoholism have an increased risk for developing pronator syndrome.
Pronator syndrome produces symptoms very similar to a more common cause of median nerve compression called “carpal tunnel syndrome”. Symptoms of pronator syndrome include numbness, tingling, or discomfort on the palm side of your thumb, index, middle finger, and half of your ring finger. The discomfort often begins near the elbow and radiates toward your hand. Your symptoms are likely aggravated by gripping activities, especially those that involve rotation of the forearm, like turning a doorknob or a screwdriver. Unlike carpal tunnel syndrome, pronator syndrome symptoms are not generally present at night. You may sometimes feel as though your hands are clumsy. In more severe cases, hand weakness can develop.
To help resolve your condition, you should avoid activities that involve repetitive hand and forearm movements. Perhaps the most important aspect of your treatment plan is to avoid repetitive forceful gripping. You may apply ice packs or ice massage directly over the pronator teres muscle for ten minutes at a time or as directed by our office. In some cases, an elbow splint may be used to limit forearm movements. If left untreated, pronator syndrome can result in permanent nerve damage. Fortunately, our office has several treatment options available to help resolve your symptoms.
Golfer’s Elbow? Thats a thing?
Most of the muscles that flex your wrist are attached to a bony bump on the inside of your elbow called the “medial epicondyle.” Sometimes, through injury or overuse, the site where these muscles originate can become irritated or inflamed. This condition is called “medial epicondylitis”, or “golfer’s elbow.”
Although the condition is named “golfer’s elbow,” over 90% of those affected

are not even athletes, much less golfers. Nonetheless, the condition is more common in certain sports, especially golf, throwing, bowling, football, archery, and weight lifting. Occupations that require heavy gripping or repeated hand movements, like carpentry or typing, can predispose you to this condition. Smokers and people who are obese are more likely to experience this condition.
Medial epicondylitis is the most frequent cause of pain on the “inside” of your elbow but is 3-10 times less likely that its “outside” counterpart- lateral epicondylitis (i.e. “tennis elbow”). Medial epicondylitis is most common between the ages of 40 and 60. The condition strikes the dominant arm in over ¾ of cases. Your symptoms will likely include a dull aching pain over the bump on the inside of your elbow that becomes more intense with use. As the condition progresses, you may notice grip weakness or limitations when shaking hands, grasping objects, and opening jars. Be sure to tell your doctor if you notice numbness or tingling traveling toward your hand.
If left untreated, medial epicondylitis can last indefinitely. Studies show that up to 40% of untreated patients suffer prolonged discomfort, some as long as three years. Fortunately, conservative treatment like the type provided in our office is effective for relieving this condition. Our office may prescribe an elbow “counterforce brace” to help dampen stress to the irritated area. This type of brace should not be used in patients who have numbness or tingling radiating into their fingers. Some patients may benefit from a “wrist splint” that is used at night to allow your tendon to heal in a lengthened position. Using ice or ice massage over your elbow can help limit pain. Your home exercises will play an important role in your recovery.
Initially, you may need to avoid activities that cause an increase in pain, like gripping, lifting, golfing, throwing balls, or swinging a racquet. Be sure to warm up properly and stretch prior to any heavy physical activity. Smokers would benefit from quitting. Overweight patients should consider increasing their aerobic activity to shed excess pounds.
How can I have Tennis Elbow? I’ve never played tennis!
Most of the muscles that extend your wrist are attached to a bony bump on the outside of your elbow called the lateral epicondyle. Sometimes, through injury or overuse, the site where these muscles insert can become irritated or inflamed. This condition is called lateral epicondylitis or “tennis elbow”- although the majority of those affected do not play tennis.

Activities involving repetitive wrist extension are a common cause of this condition, i.e., tennis, carpentry, bricklaying, knitting, playing piano, typing, or lifting objects with your palm facing down. The condition is 3 times more likely to strike your dominant arm.
The pain often begins as an intermittent or gradual discomfort during activity and progresses so that even simple activities, like holding a coffee cup, become painful. Pain may increase when you straighten your arm, grip a doorknob or shake hands. The pain may vary from mild to severe and commonly radiates into the forearm, sometimes to the wrist.
Without treatment, “tennis elbow” usually lingers – 80% of patients still report pain after one year. The first step in a successful treatment plan is to modify or eliminate activities that cause symptoms. Try to avoid lifting heavy objects with your palm facing down. Tennis or racquetball players may need to consider changing to a lighter racket or a smaller handle. We may prescribe a “counter force brace” for your elbow. This brace will act as a temporary new attachment site for your muscles thereby reducing some of the stress to your elbow. Sports creams and home ice massage may provide relief as well. Be patient with your recovery!
