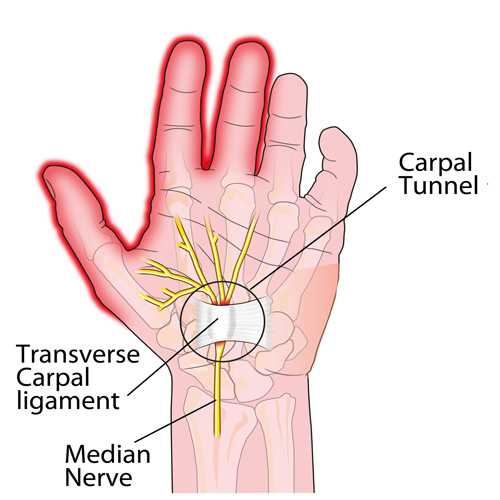
Carpal tunnel syndrome (CTS) can be an extremely painful and activity-limiting condition. It affects many people of all ages and genders, though women are affected more often than men. But how do you know if what you are suffering from is truly CTS or if it’s another condition that’s producing the symptoms in your hand or wrist?
Carpal tunnel syndrome occurs when the median nerve is compressed as it passes through the wrist. However, the median nerve travels out of the neck, through the shoulder, elbow, and forearm before it passes through the wrist and into the hand. Pinching of the median nerve ANYWHERE along its course can give rise to the signs and symptoms of CTS including numbness, tingling, and/or pain into the hand and index, third, and thumb-side half of the fourth digits, and sometimes the thumb. If the pinch is significant enough, weakness can also occur. Sometimes the median nerve can become compressed at both the wrist and other body sites as it travels from the spinal cord to your hand, that’s why it’s important for a doctor to check for impingements along the entire course of the nerve.
But compression of the median nerve isn’t the only thing that can produce symptoms in the hand. Here are a couple of the more common conditions that are often confused with CTS:
1) Ulnar neuropathy: This is pinching of the ulnar nerve (at the neck, shoulder, elbow, or wrist) but this gives rise to a similar numbness/tingling BUT into the pinky-side of the fourth and the fifth fingers (not the thumb-side of the hand). The most common pinch location is either at the neck or the inner elbow, the latter of which is called “cubital tunnel syndrome” or CuTS.
2) Tendonitis: There are a total of nine tendons that pass through the carpal tunnel that help us grip or make a fist. Similarly, there are five main tendons on the back side of the hand that allow us to open our hands and spread our fingers. ANY of these tendons can get strained or torn, which results in swelling and pain as well as limited function BUT there is usually NO NUMBNESS/TINGLING!
3) DeQuervain’s disease: This is really a tendonitis of an extensor tendon of the thumb and its synovial sheath that lubricates it resulting in a “tenosynovitis.” This creates pain with thumb movements, especially if you grasp your thumb in the palm of your hand and then bend your wrist sideways towards the pinky-side of the hand.
Chiropractors are well-trained to diagnose and treat patients with CTS. And if you don’t have CTS but another condition listed above, they can offer treatment (or a referral, if necessary) to help resolve it so you can return to your normal activities as soon as possible.