This muscle originates on the bodies and disks of T12-L5 and the inner ilium. It inserts on the lesser trochanter of the femur. The psoas flexes the hip when the spine is fixed. When the leg is fixed it extends the lumbar spine increasing lumbar lordosis. This Muscle is often chronically shortened due to inactivity and sitting posture. When trigger points are present they will refer pain primarily to the lower lumbar area and the sacrum as well as into the anterior thigh. Trigger points in the iliopsoas muscle can mimic appendicitis.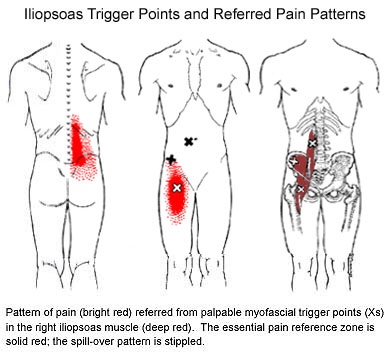
Author: bryancobb
Trigger points in the piriformis muscle
The piriformis muscle is a small muscle deep to glute max and lies over top of the sciatic nerve. It originates on the anterior sacrum, and inserts on the greater trochanter of the femur. It’s main action is to laterally rotate the femur. When trigger points developed in this muscle they will refer pain into the sacro-iliac region, across the posterior hip and down the leg. This muscle can also be a cause of sciatic nerve irritation if it gets tight, causing “sciatica” symptoms. 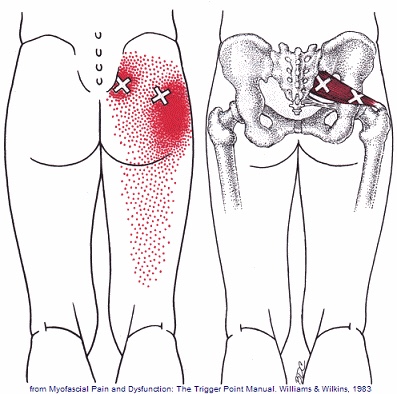
Trigger points in the gluteus minimus
The gluteus minimus is a small but important muscle that lies deep to the gluteus medius. It originates on the gluteal surface of the ilium, and attaches on the greater trochanter of the femur. It’s main actions are to abduct and medically rotate the hip. Trigger points in this muscle refer pain into the buttock and down the lateral and posterior leg, mimicking sciatica. This muscle should be the first to be examined if a straight leg test turns out negative. 
Trigger points in the gluteus medius muscle
The gluteus medius muscle plays an important role in hip and pelvic stability. It originates on the gluteal surface of the ilium, deep to the gluteus Maximus. It inserts on the greater trochanter of the femur. It’s main actions are to abduct the hip and to assist in internal rotation of the hip. It also maintains pelvic stability during walking and running. Trigger points in this muscle will refer pain into the sacrum, the iliac crest, and down the lateral hip and into the thigh. This muscle is often a cause of lower pack pain.
Trigger points in the gluteus Maximus
The gluteus Maximus is the buttock muscle. It originates on the gluteal surface of the ilium, lumbar fascia, sacrum and sacrotuberous ligament. It inserts on the gluteal tuberosity of the femur and the iliotibial tract. Extension and lateral rotation of the hip are it’s main actions. This muscle is heavily involved in activities like ice skating and is a common area to develops trigger points. When trigger points do develop they can refer pain in a crescent pattern from the gluteal fold to the sacrum. Trigger points can also refer pain deep into the buttock itself making it feel like other deeper muscles are involved. These symptoms can sometimes be mistaken for s.i. Joint problems. 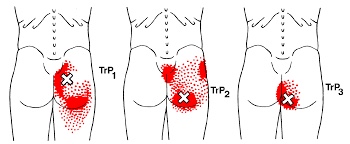
Trigger points in the supraspinatus
The supraspinatus is a muscle of the rotator cuff. Is sits above the infraspinatus and originates on the supraspinous fossa of the scapula. It’s insertion point is the superior facet of the greater tubercle of the humerus. It’s main function is to abduct the arm at the glenohumeral joint working with the deltoid. All rotator cuff muscles act to secure and support the head of the humerus in the glenoid fossa during arm movements acting as a sling. This muscle often gets impinged during overhead movements such as painting a ceiling. When trigger points form in this muscle they primarily refer a deep achy pain into the mid deltoid area with spillover pain radiating down the arm into the elbow.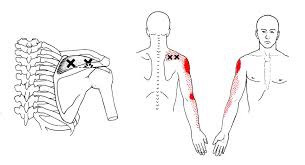
Trigger points in the infraspinatus
The infraspinatus muscle is one of the muscles that makes up the rotator cuff. It originates on the infraspinous fossa of the scapula, and inserts on the middle facet of the greater tubercle of the humerus. It functions to externally rotate the humerus and to stabilize the head of the humerus in the glenoid cavity during upward movement of the arm. Trigger points in this muscle refer pain deep into the anterior shoulder joint and down the anterior arm. Trigger points near the lower medial border refer pain into the rhomboids. This muscle is often injured during throwing motions.
Trigger points in the triceps muscle.
The tricep muscle is named for its three heads long, medial, and lateral. The long head originates on the infraglenoid tubercle, the medial head on the posterior humerus, and the lateral head on the posterior humerus as well. They join together to insert on the Olecranon process of the ulna. The triceps function to extend the elbow. Strong extension under resistance can cause trigger points to form. Pain referred from triceps trigger points can be felt in the posterior shoulder and down the posterior forearm, as well as in in the olecranon process and the lateral epicondyle which can cause “tennis elbow” pain.
Pathophysiology of trigger points.
A large number of factors have been identified as causes of trigger point activation. These include acute or chronic overload of muscle tissue, disease, psychological distress, systemic inflammation, homeostatic imbalances, direct trauma, radiculopathy, infections, and lifestyle choices such as smoking. Trigger points form as a local contraction of muscle fibres in a muscle or bundle of muscle fibres. These can pull on ligaments and tendons associated with the muscle which can cause pain to be felt deep inside a joint. It is theorized that trigger points form from excessive release of acetylcholine causing sustained depolarization of muscle fibres. Trigger points present an abnormal biochemical composition with elevated levels of acetylcholine, noradrenaline and serotonin and a lower ph. The contracted fibres in a trigger point constricts blood supply to the area creating an energy crisis in the tissue that results in the production of sensitizing substances that interact with pain receptors producing pain. When trigger points are present in a muscle there is often pain and weakness in the associated structures. These pain patterns follow specific nerve pathways that have been well mapped to allow for accurate diagnosis or the causative pain factor.
Diagnosis of trigger points.
Diagnosis of trigger points typically takes into account symptoms, pain patterns, and manual palpation. When palpating the therapist will feel for a taut band of muscle with a hard nodule within it. Often a local twitch response will be elicited by running a finger perpendicular to the muscle fibres direction. Pressure applied to the trigger point will often reproduce the pain complaint of the patient and the referral pattern of the trigger point. Often there is a heat differential in the local area of the trigger point. 
