Did you know that 50-72% of women have low back pain (LBP) and/or pelvic pain during their pregnancy but only 32% do something about it? Let’s look closer!
Pregnancy-related low back pain (PLBP) can be a highly debilitating syndrome that accounts for the most common cause of sick leave for pregnant women. In 2004, Americans spent $26.1 billion dollars in an effort to find relief from back pain during pregnancy. Statistics show one out of ten women will experience daily DISABLING LBP for at least two years following delivery.
Because of the limited number of treatment options available for the pregnant woman due to mother and fetus safety, and given the high propensity of potentially disabling PLBP that can significantly limit function and quality of life, chiropractic care seems to be a natural choice for this patient population! Obviously, pharmaceuticals and surgery are NOT appropriate options for the expectant mother, even during the post-partum breast-feeding time period. Chiropractic offers a non-invasive and safe approach to managing lumbopelvic pain that uses many different approaches.
In a 2009 research paper, 78 women participated in a study that investigated disability, pain intensity, and percent improvement after receiving chiropractic care to treat pregnancy-related PLBP. Here, 73% reported their improvement as either “excellent” or “good.” For disability and pain, 51% and 67% (respectively) experienced clinically significant improvement! Researchers followed up with them eleven months later and found 85.5% reported their improvement as either “excellent” or “good!” For disability and pain, 73% and 82% (respectively) experienced clinically significant improvement!
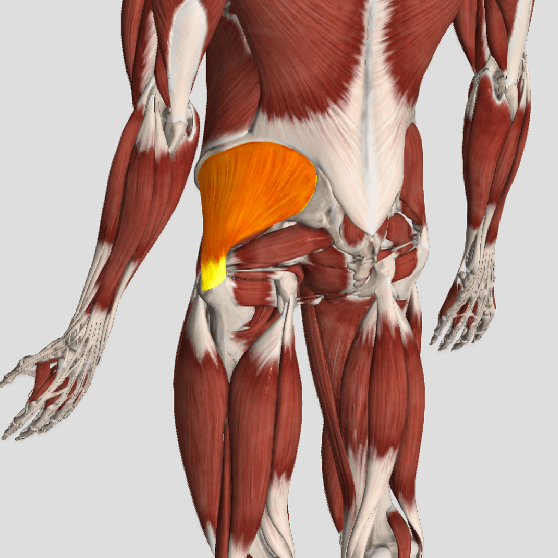
So, what’s causing LBP in pregnant women? Because of the biomechanical changes that occur in the low back and pelvis over a relatively short amount of time during pregnancy, especially in the second and third trimesters, common pain generators include (but are not limited to): the sacroiliac joint, facet joints, shock-absorbing disks, and the many connecting muscles (strains) and ligaments (sprains). During the later stages of pregnancy, the hormone Relaxin prepares the pelvis for delivery by widening the pelvic girdle, which can also be problematic.
Treatment options within chiropractic often include spinal manipulation, lumbopelvic exercises, patient education, posture correction, massage, an SI belt, soft tissue mobilization, and more. Exercises that target the transverse abdominus, multifidus, and pelvic floor muscles help to stabilize the lumbopelvic region. The American College of Obstetricians & Gynaecologists recommends exercise at least three times a week during pregnancy, and studies report NO obstetric complications (pre-term labor, premature ruptured membranes, or changes to maternal or neonatal weight) with exercise.
So, the answer is clear! When PLBP strikes, seek chiropractic care to safely and effectively manage the pain and disability and so you can ENJOY YOUR PREGNANCY!!!
We realize you have a choice in whom you consider for your health care provision and we sincerely appreciate your trust in choosing our service for those needs. If you, a friend, or family member requires care for back pain, we would be honoured to render our services.