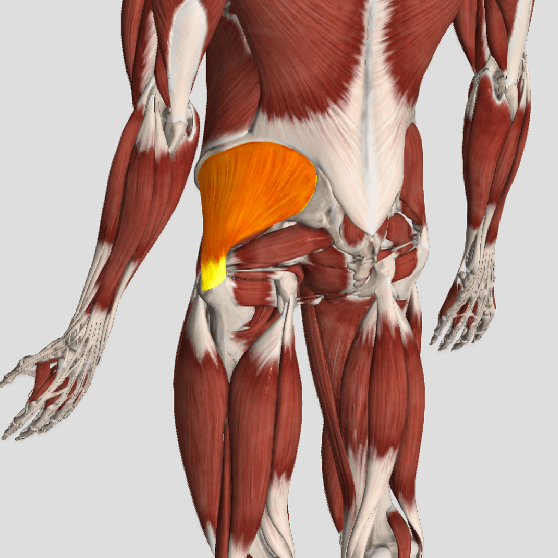
Technically, the hip is the ball-and-socket joint between the long bone of the thigh and the pelvis; but more often than not, many people will point to a number of different places on their back or pelvis and say, “My hip is killing me” when it’s not really “the hip” at all!
Hip pain can be located in the front (groin area), the side, the back, or in the buttocks. The “classic sign” of hip pain is reproduced most consistently when you try to cross your legs—put your ankle on the far end of the thigh and then push down on your knee. This may feel tight and cause pain in the groin area. For many people, hip pain is also reproduced when they cross their legs and then pull their knee towards the opposite shoulder.
The hip is a VERY strong joint due to the deep receiving cup of the pelvis and the round ball that fits nicely into it. Because it’s a freely moving joint, there is a joint capsule. The capsule is lined with tissue that produces an oily substance that lubricates the joint (called synovial fluid), and when hip pain occurs, this can be caused by a capsulitis (inflammation of the capsule) with a buildup of synovial fluid (called synovitis).
When the smooth, shiny surface of the ball starts to wear thin (which can eventually wear away down to the bone), that’s a condition called “osteoarthritis.” This occurs over time for many and may eventually result in the need for a hip replacement. This usually isn’t needed until an individual is in their late 60s or older (if at all), but for those who injure a hip earlier in life, the “wearing out” process may accelerate and a hip replacement may be needed well before old age.
There are many studies that report low back and hip arthritis often occur together, and differentiating between the two can sometimes be a challenge. For example, pain can radiate from the hip to the knee, which many doctors will diagnose as “sciatic nerve.” But hip pain can present exactly the same, making it hard to determine if it’s low back-generated pain or hip-generated pain.
This is why it’s SO IMPORTANT that your doctor of chiropractic conduct a careful history and examination. There are specific tests that he or she will perform that help determine which of the two is causing the pain. There are times when they may find BOTH problems co-existing together, making it necessary to manage two problems, rather than just one.
There are many mobilization, manipulation, soft tissue therapies, modalities, and exercises available to patients with both hip and low back pain. So if you’re not sure what is bothering you and you don’t know what to do, visit your doctor of chiropractic and he or she will help you through this.
Uncategorized
What Is Facet Syndrome?

As stated in previous articles, low back pain (LBP) can arise from many different structures. Lumbar facet syndrome is one that involves the facet joint and includes both acute (new) and chronic (old) varieties. The facet joint is synonymous with the zygapophyseal joint, so if you hear that word, don’t let it throw you off! Approximately 45% of patients with chronic low back pain suffer from “facet syndrome” (FS) in which the facets are the low back pain generator.
There are many conditions that give rise to FS. Some of these include the straining of the surrounding joint capsule (the capsule holds the joint securely together), joint hypomobility (reduced motion in the joint), a synovial cyst (similar to a ganglion on the back of the wrist but its located inside the joint), and degeneration (also called osteoarthritis—the wearing out type of arthritis).
Because facet syndrome can accompany other conditions, a doctor of chiropractic must evaluate each patient individually and manage each person appropriately. In “pure” facet syndrome, pain rarely ever passes the level of the knee and does not cause neurological loss (weakness, loss of reflex, etc.). It can create numbness but usually NOT beyond the knee. Pain is usually not worsened by hip movements such as straight leg raise or hip rotation.
The facet joint’s “job” (at least in part) is to limit or guard twisting movements in the upper lumbar/low back region, and the lower lumbar facets are shaped to limit motion when bending forwards and backwards. Facet joints are unique because they are innervated by specific nerves that can be blocked by injecting an anesthetic agent to determine if the facet (and its innervating nerve) is the main source of pain. The surrounding capsule around the facet joint contains mechanoreceptors (cells that detect movement) and nociceptors (cells that detect pain) that fire when the facet joint is compressed/jammed or over-stretched. These nociceptors can become “hypersensitized” (very irritable) when they remain inflamed over time.
In many patients, injury to a facet joint is the result of many microtraumas over a period of time and not one single isolated event. For example, repeatedly bending backwards, twisting, and leaning to one side can stretch the joint capsule and fatigue it until some capsular tissues finally “give” and it inflames which generates pain.
These joints commonly become arthritic with age, which is one reason people over 50-60 years old commonly present with FS. Osteoarthritis results in a narrowing of the joint space and causes a more permanently “jammed” joint. This is one reason many elderly people walk partially bent over—as bending forwards opens the facet joints and “feels good!”
The good news is that chiropractic manipulation is a highly effective treatment for facet syndrome, and most patients feel much better within the first or second week of care (often within three to five visits).
What is causing my LBP?
 Low back pain (LBP) can arise from disks, nerves, joints, and the surrounding soft tissues. To simplify the task of determining “What is causing my LBP?” the Quebec Task Force recommends that LBP be divided into three main categories:
Low back pain (LBP) can arise from disks, nerves, joints, and the surrounding soft tissues. To simplify the task of determining “What is causing my LBP?” the Quebec Task Force recommends that LBP be divided into three main categories:
1) Mechanical LBP
2) Nerve root related back pain and
3) Pathology or fracture. We will address the first two, as they are most commonly managed by chiropractors.
Making the proper diagnosis points your doctor in the right direction regarding treatment. It avoids time wasted by treating an unrelated condition, which runs the risk of increased chances of a poor and/or prolonged recovery. Low back pain is no exception! The “correct” diagnosis allows treatment to be focused and specific so that it will yield the best results.
Mechanical low back pain is the most commonly seen type of back pain, and it encompasses pain that arises from sprains, strains, facet and sacroiliac (SI) syndromes, and more. The main difference between this and nerve root-related LBP is the ABSENCE of a pinched nerve. Hence, pain typically does NOT radiate, and if it does, it rarely goes beyond the knee and normally does not cause weakness in the leg.
The mechanism of injury for both types of LBP can occur when a person does too much, maintains an awkward position for too long, or over bends, lifts, and/or twists. However, LBP can also occur “insidiously” or for seemingly no reason at all. However, in most cases, if one thinks hard enough, they can identify an event or a series of “micro-traumas” extending back in time that may be the “cause” of their current low back pain issues.
Nerve root-related LBP is less common but it is often more severe—as the pain associated with a pinched nerve is often very sharp, can radiate down a leg often to the foot, and cause numbness, tingling, and muscle weakness. The location of the weakness depends on which nerve is pinched.
Think of the nerve as a wire to a light and the switch of the nerve is located in the back where it exits the spine. When the switch is turned on (the nerve is pinched), and the “light” turns on—possibly in the outer foot, middle foot, inner foot, or front, back or side of the thigh. In fact, there are seven nerves that innervate or “run” into our leg, so usually, a very specific location “lights up” in the limb.
Determining the cause of your low back pain helps your doctor of chiropractic determine which treatments may work best to alleviate your pain as well as where such treatments can be focused.
Those “other” causes of back pain

Between 80% and 90% of the general population will experience an episode of lower back pain (LBP) at least once during their lives. When it affects the young to middle-aged, we often use the term “non-specific LBP” to describe the condition. The geriatric population suffers from the “aging effects” of the spine—things like degenerative joint disease, degenerative disk disease, and spinal stenosis. Fractures caused by osteoporosis can also result in back pain.
The “good news” is that there are rare times when your doctor must consider a serious cause of LBP. That’s why he or she will ask about or check the following during your initial consultation:
1) Have you had bowel or bladder control problems? (This is to make sure a patient doesn’t have “cauda equina syndrome”—a very severely pinched nerve.)
2) Take a patient’s temperature and ask about any recent urinary or respiratory tract
infections to rule out spinal infections.
3) To rule out cancer, a doctor may ask about a family or personal history of cancer, recent unexplained weight loss, LBP that won’t go away with time, or sleep interruptions that are out of the ordinary.
4) To rule out fractures, a doctor may also take x-rays if a patient is over age 70 regardless of trauma due to osteoporosis, over age 50 with minor trauma, and at any age with major trauma.
Once a doctor of chiropractic can rule out the “dangerous” causes of LBP, the “KEY” form of treatment is giving reassurance that LBP is manageable and advise LBP sufferers of ALL ages (especially the elderly) to KEEP MOVING! Of course, the speed at which we move depends on many things—first is safety, but perhaps more importantly is to NOT BECOME AFRAID to do things! As we age, we gradually fall out of shape and end up blaming our age for the inability to do simple normal activities. Regardless of age, we must GRADUALLY increase our activities to avoid the trap of sedentary habits resulting in deconditioning followed “fear avoidant behavior!”
Here are a few “surprising” reasons your back may be “killing you”:
1) You’re feeling down – That’s right, having “the blues” and more serious mood disorders, like depression, can make it more difficult to cope with pain. Also, depression often reduces the drive to exercise, may disturb sleep, and can affect dietary decisions—all of which are LBP contributors.
2) Your phone – Poor posture caused by holding a phone between your bent head and shoulder (get a headset!) or prolonged mobile phone use can increase your risk for spinal pain.
3) Your feet hurt, which makes you walk with an altered gait pattern, forcing compensatory movements up the “kinetic chain” leading to LBP.
4) Core muscle weakness, especially if you add to that a “pendulous abdomen” from being overweight—this is a recipe for disaster for LBP.
5) Tight short muscles such as hamstrings, hip rotator muscles, and/or tight hip joint capsules are common problems that contribute to LBP. Stretching exercises can REALLY help!
10 tricks to help LBP

Low back pain (LBP) is VERY likely to affect all of us at some point in life. The question is, do you control IT or does IT control you? Here are ten “tricks” for staying in control of “IT!”
1) STRETCH: When you’re in one position for a long time (like sitting at your desk), SET your cell phone timer to remind yourself to get moving and stretch every 30-60 minutes! Mornings are a great time to stretch.
2) BE SMART: Do NOT place your computer monitor anywhere other than directly in front of you. Shop carefully for a GOOD supportive office chair that is comfortable and a good fit.
3) POSTURE: For sitting, sit as upright as comfortably possible keeping your chin tucked in so the head stays back over the shoulders.
4) SHOE WEAR: Avoid wearing heels greater than one inch high (2.54 cm). A supportive shoe that can be worn COMFORTABLY for several hours is ideal! Generally, the “skimpier” the shoe, the worse the support, so don’t “skimp” on shoe wear!
5) SMOKING: Carbon monoxide from cigarette smoke competes with oxygen at each cell in the body literally suffocating them, which makes the healing process more difficult.
6) WEIGHT: Your body mass index (BMI) should be between 18.5 and 25. Search the internet for “BMI Calculator” and plug in your height and weight to figure out yours. BMI is a reliable indicator of body fatness and a great way to determine where you are at for goal setting.
7) ANTI-INFLAMMATION: Common over the counter (OTC) medications include ibuprofen and naproxen. However, recent studies show these types of medications (NSAIDS) may delay the healing process. A healthier choice is ginger, turmeric, and bioflavonoids, which are commonly bundled together in a supplement. Eat fresh fruits, veggies, lean meats, and food rich in omega-3 fatty acids. Vitamin D, magnesium, and coenzyme Q10 are also smart choices. AVOID FAST FOOD as they tent to be rich in omega-6 fatty acids, which can promote inflammation.
8) ICE: This could be included in #7 but deserves its own space. Ice reduces swelling while heat promotes it. Try rotations of ice every 15-20 minutes for about an hour three times a day to “pump” out the swelling!
9) STAY ACTIVE: Balance rest with physical activity like exercise or simply going for a walk. The most important thing is to move your body around.
10) STRENGTHEN: Core stabilizing exercises (sit-ups, planks, quadruped) and BALANCE exercises are VERY important!
Where does back pain come from?
Most of us have suffered from back pain at one time or another. It often occurs after over-doing a physical task, like fall yard work, winter snow shoveling, working on the car, cleaning the house, and so on. But there are times when identifying the cause of back pain can be difficult or impossible. Let’s take a deeper look at where back pain can come from…
Though activity-related back pain is common, many times a direct link to over-use is not clear. Micro-traumatic events can accumulate and become painful when a certain threshold is exceeded. (Think of the old adage “The straw that broke the camel’s back.”)
There are other less well-identified causes of back pain. One is called referred pain. This can be caused by an irritated joint or soft tissue not necessarily located in the immediate area of the perceived pain. For example, pain in the leg can result from an injured facet joint, sacroiliac joint, and/or a disk tear (without nerve root pinch). This is called “sclertogenous pain.”
Internal organs can also cause back pain. This is called a “viscerosomatic response” (VSR). A classic example of this is when the right shoulder blade seems to be the source of pain when the gall bladder is inflamed. This pain can be located at or below the scapula next to the spine and the muscles in the area are in spasm and sensitive or painful to the touch. Also, VSR is often not worsened or changed by bending in different directions (unlike musculoskeletal / MSK pain). Without further testing, it’s easy to confuse this with a MSK or a “typical” back ache. Ultimately, a final diagnosis may require an abdominal ultrasound (CT, MRI scan, and other diagnostics are less frequently used).
Visceral pathology in the back pain patient presenting to chiropractors is reportedly rare, and according to one survey, only 5.3% of patients present with non-musculoskeletal complaints. Other common VSR pain patterns are as follows: Heart – left chest to left arm, mid-upper back, left jaw; Liver – right upper shoulder (front and back), right middle to low back, and just below the sternum; Appendix – right lower abdomen (may start as stomach pain); Small intestine – either side of the umbilicus and/or between it and the breast bone; Kidney – small of the back, upper tailbone, and/or groin area; Bladder – just above the pubic bone and/or bilateral buttocks; Ovaries – groin and/or umbilical area; and Colon – mid-abdominal and/or lower quadrants.
Another challenge to diagnosis is cancer in the spine, which can be primary or metastatic (from a different location). Thankfully, this is very rare. A history of unexplained weight loss, a past history of cancer, over age 50, nighttime sleep interruptions, and no response to usual back care may lead a doctor to recommend tests to determine if cancer is present in the spine.
Bottom line: When patients present with back pain, chiropractors have been trained to look for these less common but important causes of back pain. They get “suspicious” when the “usual” orthopedic tests do not convey the usual responses seen with mechanical back pain. In these cases, they work with primary care doctors to coordinate care to obtain prompt diagnostic testing and treatment.
We realize you have a choice in whom you consider for your health care provision and we sincerely appreciate your trust in choosing our service for those needs. If you, a friend, or family member requires care for back pain, we would be honored to render our services.
Why does my back hurt?

It’s been said that if you haven’t had back pain, just wait, because (statistically) some day you will! The following list is a list of “causes” that can be easily “fixed” to reduce your risk for a back pain episode.
1. MATTRESS: Which type of mattress is best? The “short answer”: there is no single mattress (style or type) for all people, primarily due to body type, size, gender, and what “feels good.” TRY laying on a variety of mattresses (for several minutes on your back and sides) and check out the difference between coiled, inner springs, foam (of different densities), air, waterbeds, etc. The thickness of a mattress can vary from 7 to 18 inches (~17-45 cm) deep. Avoid mattresses that feel like you’re sleeping in a hammock! A “good” mattress should maintain your natural spinal curves when lying on your sides or back (avoid stomach sleeping in most cases). Try placing a pillow between the knees and “hug” a pillow when side sleeping, as it can act like a “kick stand” and prevent you from rolling onto your stomach. If your budget is tight, you can “cheat” by placing a piece of plywood between the mattress and box spring as a short-term fix.
2. SHOES: Look at the bottom of your favorite pair of shoes and check out the “wear pattern.” If you have worn out soles or heels, you are way overdue for a new pair or a “re-sole” by your local shoe cobbler! If you work on your feet, then it’s even more important for both managing and preventing LBP!
3. DIET: A poor diet leads to obesity, which is a MAJOR cause of LBP. Consider the Paleo or Mediterranean Diet and STAY AWAY from fast food! Identify the two or three “food abuses” you have embraced and eliminate them – things with empty calories like soda, ice cream, chips… you get the picture! Keeping your BMI (Body Mass Index) between 20 and 25 is the goal! Positive “side-effects” include increased longevity, better overall health, and an improved quality of life!
4. EXERCISE: The most effective self-help approach to LBP management is exercise. Studies show those who exercise regularly hurt less, see doctors less, have a higher quality of life, and just feel better! This dovetails with diet in keeping your weight in check as well. Think of hamstring stretches and core strengthening as important LBP managers – USE PROPER TECHNIQUE AND FORM; YOUR DOCTOR OF CHIROPRACTIC CAN GUIDE YOU IN THIS PROCESS!
5. POSTURE: Another important “self-help” trick of the trade is to avoid sitting slumped over with an extreme forward head carriage positions. Remember that every inch your head pokes forwards places an additional ten pounds (~4.5 kg) of load on your upper back muscles to keep your head upright, and sitting slumped increases the load on your entire back!
We have only scratched the surface of some COMMON causes and/or contributors of back pain. Stay tuned next month as we continue this important conversation!
We realize you have a choice in whom you consider for your health care provision and we sincerely appreciate your trust in choosing our service for those needs. If you, a friend, or family member requires care for back pain, we would be honored to render our services.
How Common Is Low Back Pain?

Low back pain (LBP) is a very common problem that affects most of us at some point in life and for some, it’s a daily issue. Through education and research, researchers have found low back-specific exercises can not only help get rid of LBP but can also prevent future exacerbations or episodes. Like brushing our teeth, low back exercises are equally important in order to maintain, preserve, and optimize function. But because there are SO MANY exercise options available, it’s hard to know which ones are best, especially for each specific person.
There are different methods for determining the right low back exercises for the patient. One of the most common is to try different exercises to determine individual tolerance, but this is not very specific, as it only determines whether or not the patient is comfortable with an exercise. Another is using physical performance tests (PPTs) that measure the strength and endurance of specific muscle groups, muscle shortness, balance, aerobic capacity, and spinal range of motion.
Physical performance tests are much more specific because they address each patient’s differences. Also, many PPTs include normative data to compare against the patient’s own performance, so repeat use of the abnormal PPTs on a monthly interval can gauge their progress (or the lack thereof), which is motivating to the patient and serves as a great outcome measure!
PPTs are typically done two to four weeks after an initial presentation or at a time when the condition is stable so as not to irritate the condition. Initially, the decision as to which exercise is best is often made by something called “directional preference” or positional bias. This simply means if a patient feels best by bending over, we initially give “flexion-biased” exercises.
Flexion-biased exercises include (partial list): pulling the knees to the chest (single then double), posterior pelvic tilts (flattening the low back into the floor), sitting and/or standing bend overs, hamstring stretches, and more. If a person’s low back feels best bending backwards, their doctor of chiropractic may give extension-biased exercises, which include (partial list): standing back bends, saggy push-ups (prone press-ups), and/or laying on pillows or a gym ball on their back, arching over the ball.
Chiropractors generally add exercises gradually once they’ve determined tolerance and will recheck to make sure the patient is doing them correctly. Studies show that spinal manipulation achieves great short-term results, but when exercise is added to the treatment plan, the patient can achieve a more satisfying long-term result.
Unfortunately, other studies have shown that ONLY 4% of patients continue their exercises after pain is satisfactorily managed and they fall back into old habits of not exercising.
MRI Truths & Myths 

Low back pain is a very common complaint. In fact, it’s the #1 reason for doctor visits in the United States! The economic burden of LBP on the working class is astronomical. Most people can’t afford to be off work for one day, much less a week, month, or more! Because of the popularity of hospital-based TV dramas over the past two decades, many people think getting an MRI of their back can help their doctor fix their lower back problem. Is this a good idea? Let’s take a look!
Patients will often bring in a CD that has an MRI of their lower back to a doctor of chiropractic and ask the ultimate question, “….can you fix me?” Or, worse, “…I think I need surgery.” Sure, it’s quite amazing how an MRI can “slice” through the spine and show bone, soft tissues, disks, muscles, nerves, the spinal cord, and more! Since the low back bears approximately 2/3 of our body’s weight, you can frequently find MANY ABNORMALITIES in a person over 40-50 years old. In fact, it would be quite odd NOT to see things like disk degeneration, disk bulges, joint arthritis, spur formation, etc.!
Hence, the “downside” of having ALL this information is the struggle to determine which finding on the MRI has clinical significance. In other words, where is the LBP coming from? Is it that degenerative disk, bulged disk, herniated disk, or the narrowed canal where the nerve travels? Interestingly, in a recent review of more than 3,200 cases of acute low back pain, those who had an MRI scan performed earlier in their care had a WORSE outcome, more surgery, and higher costs compared with those who didn’t succumb to the temptation of requesting an MRI!
This is not to say MRI, CT scans, and x-rays are not important, as they effectively show conditions like subtle fractures and dangerous conditions like cancer. But for LBP, MRI is often misleading. This is because the primary cause of LBP is “functional” NOT “structural,” so it’s EASY to get railroaded into thinking whatever shows up on that MRI has to be the problem.
Here is how we know this, when we take 1,000 people WITHOUT low back pain between ages 30 and 60 (male or female) and perform an MRI on their lower back, we will find up to 53% will have PAINLESS disk bulges in one or more lumbar disks. Moreover, we will find up to 30% will have partial disk herniations, and up to 18% will have an extruded disk (one that has herniated ALL the way out). Yet, these people are PAIN FREE and never knew they had disk “derangement” (since they have no LBP). When combining all of these possible disk problems together, several studies report that between 57% and 64% of the general population has some type of disk problem without ANY BACK PAIN!
Hence, when a patient with a simple sprain/strain and localized LBP presents with an MRI showing a disk problem, it usually ONLY CONFUSES the patient (and frequently the doctor), as that disk problem is usually not the problem causing the pain! So DON’T have an MRI UNLESS a surgical treatment decision depends on its findings. That is weakness, numbness, and non-resolving LBP in spite of 4-6 weeks of non-surgical care or unless there is weakness in bowel or bladder control. Remember, the majority of back pain sufferers DO NOT need surgery!
We realize you have a choice in whom you consider for your health care provision and we sincerely appreciate your trust in choosing our service for those needs. If you, a friend, or family member requires care for back pain, we would be honored to render our services.
LBP & Pregnancy

Did you know that 50-72% of women have low back pain (LBP) and/or pelvic pain during their pregnancy but only 32% do something about it? Let’s look closer!
Pregnancy-related low back pain (PLBP) can be a highly debilitating syndrome that accounts for the most common cause of sick leave for pregnant women. In 2004, Americans spent $26.1 billion dollars in an effort to find relief from back pain during pregnancy. Statistics show one out of ten women will experience daily DISABLING LBP for at least two years following delivery.
Because of the limited number of treatment options available for the pregnant woman due to mother and fetus safety, and given the high propensity of potentially disabling PLBP that can significantly limit function and quality of life, chiropractic care seems to be a natural choice for this patient population! Obviously, pharmaceuticals and surgery are NOT appropriate options for the expectant mother, even during the post-partum breast-feeding time period. Chiropractic offers a non-invasive and safe approach to managing lumbopelvic pain that uses many different approaches.
In a 2009 research paper, 78 women participated in a study that investigated disability, pain intensity, and percent improvement after receiving chiropractic care to treat pregnancy-related PLBP. Here, 73% reported their improvement as either “excellent” or “good.” For disability and pain, 51% and 67% (respectively) experienced clinically significant improvement! Researchers followed up with them eleven months later and found 85.5% reported their improvement as either “excellent” or “good!” For disability and pain, 73% and 82% (respectively) experienced clinically significant improvement!
So, what’s causing LBP in pregnant women? Because of the biomechanical changes that occur in the low back and pelvis over a relatively short amount of time during pregnancy, especially in the second and third trimesters, common pain generators include (but are not limited to): the sacroiliac joint, facet joints, shock-absorbing disks, and the many connecting muscles (strains) and ligaments (sprains). During the later stages of pregnancy, the hormone Relaxin prepares the pelvis for delivery by widening the pelvic girdle, which can also be problematic.
Treatment options within chiropractic often include spinal manipulation, lumbopelvic exercises, patient education, posture correction, massage, an SI belt, soft tissue mobilization, and more. Exercises that target the transverse abdominus, multifidus, and pelvic floor muscles help to stabilize the lumbopelvic region. The American College of Obstetricians & Gynecologists recommends exercise at least three times a week during pregnancy, and studies report NO obstetric complications (pre-term labor, premature ruptured membranes, or changes to maternal or neonatal weight) with exercise.
So, the answer is clear! When PLBP strikes, seek chiropractic care to safely and effectively manage the pain and disability and so you can ENJOY YOUR PREGNANCY!!!
We realize you have a choice in whom you consider for your health care provision and we sincerely appreciate your trust in choosing our service for those needs. If you, a friend, or family member requires care for back pain, we would be honored to render our services.
